.jpg)
Universal Health Coverage: How Can It Help & How Can We Achieve It?
- Aug 8, 2021
- 6 min read
Updated: Sep 8, 2021

"Universal health coverage is the single most powerful concept that public health has to offer. It is our ticket to greater efficiency and better quality. It is our savior from the crushing weight of chronic noncommunicable diseases that now engulf the globe."
— Margaret Chan, WHO Director General, 65th World Health Assembly, Geneva, Switzerland (May 23, 2012)
What is Universal Health Coverage (UHC) & Why Do We Need It?
According to the World Health Organization (WHO) , Universal Health Coverage (UHC) means “all individuals and communities receive the health services they need without suffering financial hardship.” UHC is expanded to include the “full spectrum of essential, quality health services, from health promotion to prevention, treatment, rehabilitation, and palliative care across the life course.”
Half of the world’s population does not have access to necessary healthcare.
Over 930 million people spend at least 10% of their entire household income on healthcare.
100 million people are driven into poverty each year because of out-of-pocket health spending.
According to the WHO, in 2017, 6 million women and children could have been saved worldwide if they simply had access to basic and essential healthcare.
Health is a human right. UHC is necessary to ensure equity in access to health services. Doing so protects the health of society's most vulnerable members. Furthermore, it ensures that individuals are protected against financial harm by ensuring public health services are not paid out-of-pocket.
How do countries achieve UHC? This article will first highlight the 3 common features observed across all countries that have achieved UHC, followed by an exploration of the historical, political and economic trends associated with those features.
Common Patterns in Countries That Have Achieved Universal Health Coverage
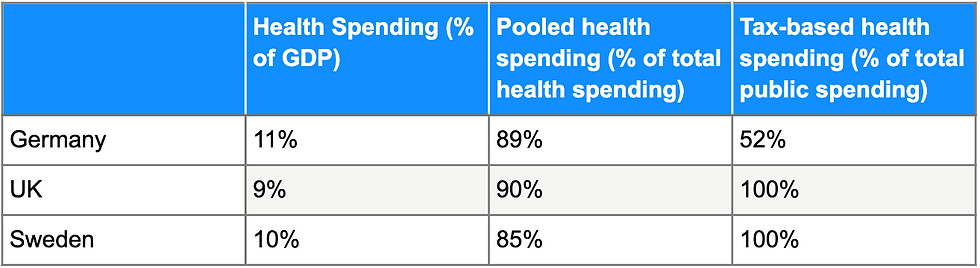
UHC is broadly defined in terms of rights to health care, financial protections, and ability to utilize healthcare services. Although it can be achieved through varying financing systems and political processes, there are historically 3 common features within the countries that have successfully implemented UHC.
Political processes driven by social force to create equitable public programs and policies.
Growth in income and rise in health spending.
Pooled spending on healthcare rather than individuals paying out-of-pocket. This is often seen in the form of taxes or mandatory insurance schemes. (This is the most necessary, but not sufficient, condition for achieving UHC)
Political & Historical Trends
Countries that have achieved UHC show 4 common political and historical patterns:
1.They achieve UHC due to widespread and persistent social pressures.
This form of domestic pressure can come in many forms i.e., citizens are concerned about rising costs of healthcare, health professionals are concerned about public health, or unions want to protect workers rights and demand better services. An early example of such a trend was seen in early 19th century Japan where villages created collective associations for healthcare funding called jyorei.
2. Governments are the dominant force in implementing UHC, although the form of this role may vary.
Empirical studies have shown that public approaches led by governments, rather than private approaches to healthcare, are often better at protecting citizens and promoting a better quality of care. They are able to pool taxes, or establish necessary insurance schemas.
3. UHC is only achieved through negotiation, debates and dialogue.
UHC is often the outcome of politics and national debate. Despite an overwhelming trend towards UHC worldwide, implementation efficiency varies between countries according to the ability of citizens to engage in public discussion or discourse. This discussion or discourse is often affected by the level of political censorship within countries. It is influenced by political institutions that filter and channel certain interests. Oftentimes, UHC emerged as a result of compromise and struggle. For example, the 19th century German health insurance system was the result of compromise between Chancellor Otto von Bismarck and the political opposition.
4. Achieving UHC takes time.
Incorporating different subgroups of the population into UHC is a gradual process. Additionally, debates are never-ending and will continue in response to changes in economics, politics, new medical technology, or persistent inequities. The first to achieve UHC are often employees of large or small firms, followed by rural workers, the self-employed, and eventually the unemployed. Healthcare systems often take time to expand from urban centers to more rural areas. The range of new healthcare services also tends to grow over time.
Economic Trends
Economic growth generates both resources and demand for more healthcare services. Most healthcare systems originate in out-of-pocket services due to a general low demand for health services. As countries grow economically, a country’s health sending increases as well with pooled financing becoming the dominant mechanism for health spending. How does increased health spending promote the implementation of UHC?
1. Income
Increased income increases effective demand for healthcare services. It is important to note that some of this demand is offset by the direct effect of higher income on improved health i.e. greater access to food and sanitation. As households grow wealthier, they are able to spend more on health care and health insurance, and can be mandated to make larger contributions to the taxation pool. Governments in higher income countries in turn can invest more money into improved public health services. On average, a 1% increase in national income is associated with nearly a 9% increase in health spending.
2. Changing Medical Practices
As technological innovation flourishes over time, our ability to prevent and treat more illnesses rise as well. With greater access to medical drugs, diagnostics and procedures, a nation's health spending increases well. Studies have shown that new medical technologies account for nearly two-thirds of the growth in health spending in countries such as France.
3. Pooled Financing
Pooled financing is a factor that promotes UHC. Firstly, it increases the demand for higher health spending by increasing the effective demand for healthcare services. Pooled financing allows poorer households to gain access to services they would otherwise not have access to. Secondly, pooling allows for more cost-effective services. By pooling funds, institutions can negotiate fees and prices, set global budgets, or restructure insurance provider payments to encourage efficient care. Pooled financing more effectively removes financial barriers that prevent citizens from accessing necessary healthcare services.,
Implications for Achieving UHC
Countries of all income levels are pursuing UHC. Middle to high income countries are still improving their systems to address remaining inequities, inefficiencies, and cost-effectiveness. Low to middle income countries are still in the process of policy reform and resource mobilization. These countries face unique challenges.
Epidemiological challenges, especially in the context of COVID-19, pose a more serious threat to such countries. This is especially considering that they have generally faster-growing populations and a higher prevalence of infectious diseases.
However, today's modern age has allowed many countries to learn from the failures and successes of their predecessors who have already achieved UHC, in a shorter amount of time and with fewer resources no less:
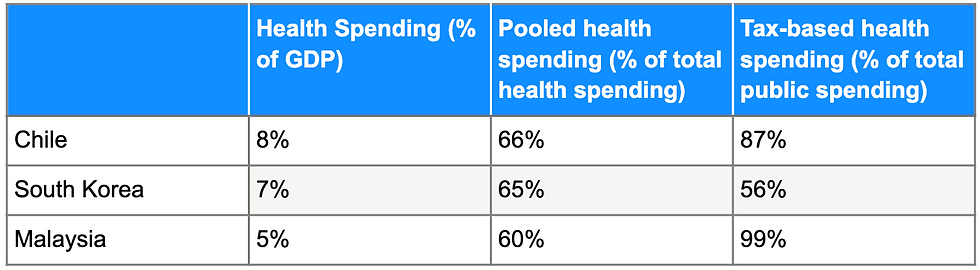
Both Malaysia and South Korea have managed to reach UHC in 2-3 decades even with lower national income levels than the countries that preceded them. Pooling funds in Malaysia are generated almost entirely through general taxes, while South Korea pools its funds through payroll contributions.
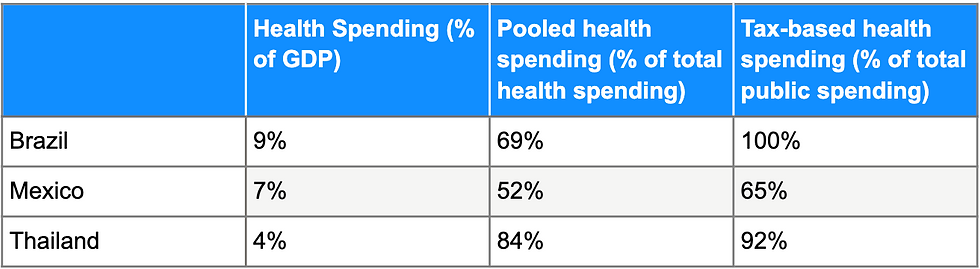
Other low to middle income countries are showing great progress in achieving UHC gradually:
National health insurance schemes are already being implemented in countries such as Ghana, Colombia, and Indonesia.
China, a country that had initially privatized its healthcare sector, has since learned the benefits of UHC and is expanding insurance coverage through public programs.
Why is the US Unique Among High-Income Countries?
The US remains a special outlier among high income countries. Despite persistent domestic pressure for UHC, only partial initiatives to extend health coverage to more citizens have succeeded so far i.e. the Stage Children’s Health Insurance Program and the Affordable Care Act. While the US has shown great progress in generalizing access to healthcare since the 1960s, 50% of its health spending is still privatized.

Mandatory health coverage (the individual mandate that required almost all Americans to have health insurance coverage or pay a penalty) was ultimately enacted in 2010 under the Obama administration's Affordable Care Act. While this establishes the basic principle of UHC in its laws, it is still several steps behind other high income countries across the globe.

It is even more important to note that the Tax Cut and Jobs Act of 2017 signed into law during the Trump administration cancelled the penalty enforced by the Affordable Care Act’s individual mandate beginning in 2019. Without a penalty, the individual mandate requiring Americans to have healthcare has effectively been rendered moot, leaving health coverage in a precarious state in the US once again.
What do countries need to achieve UHC?
UHC can be achieved at low costs if countries choose to allocate resources in the most cost-effective ways possible. This feat is not limited solely to high-income countries.
By recognizing the importance of political action in promoting health spending through pooled financing mechanisms, countries can successfully promote equitable and efficient healthcare.
By identifying and mobilizing groups or institutions that desire UHC, countries can negotiate public roles that are compatible with their own political institutions, and take advantage of cost-effective strategies to extend healthcare access to everyone.
Sources
Primary Article
Title: Political and economic aspects of the transition to universal health coverage.
Authors: William D Savedoff, David de Ferranti, Amy L Smith, Victoria Fan
Year: 2012
Journal: The Lancet
Savedoff, W. D., de Ferranti, D., Smith, A. L., & Fan, V. (2012). Political and economic aspects of the transition to universal health coverage. The Lancet, 380(9845), 924–932. https://doi.org/10.1016/s0140-6736(12)61083-6
Schmidt, H., Gostin, L. O., & Emanuel, E. J. (2015). Public health, universal health coverage, and Sustainable Development Goals: can they coexist? The Lancet, 386(9996), 928–930. https://doi.org/10.1016/s0140-6736(15)60244-6
Universal health coverage (UHC). (2021, April 1). World Health Organization. https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc)
The Effect of Eliminating the Individual Mandate Penalty and the Role of Behavioral Factors. (2018, July 11). Commonwealth Fund. https://www.commonwealthfund.org/publications/fund-reports/2018/jul/eliminating-individual-mandate-penalty-behavioral-factors



Comments